To: Centers for Disease Control and Prevention (CDC)
From: Morgellons Research Foundation
Date: February 14, 2006
Subject: CASE DEFINITION – MORGELLONS DISEASE (DRAFT)
The following case definition of Morgellons disease has been developed by physicians on the medical advisory board of the Morgellons Research Foundation. This case definition is a preliminary and evolving document, now updated for review by the Centers for Disease Control and Prevention (CDC). This document will be refined as further information becomes available and as members of the medical advisory board deem necessary.
The Following Six Signs or Symptoms Are The Basis of Morgellons Disease
1. Skin lesions, both spontaneously appearing and self-generated, with intense itching. The former may initially appear as “urticarial-like”, or as “pimple-like” with or without a white center. The latter appear as linear or “picking” excoriations. Even when not self-generated, lesions often progress to open wounds that heal abnormally and usually incompletely. (e.g., heal very slowly with discolored epidermis or seal over with a thick gelatinous outer layer.)
2. Crawling sensations, both within and on the skin surface. Often conceptualized by the patient as “bugs moving, stinging or biting” intermittently. Besides the general dermis, may also involve the scalp, nares, ear canal, and body hair or hair follicles. The sensations are at times related to the presence of easily seen insects, arthropods, and other human and non-human associated parasites that require serious attention from the observing clinician.
3. Fatigue significant enough to interfere with the activities for daily living.
4.Cognitive difficulties, including measurable short term memory and attention deficit, as well as difficulty processing thoughts correctly. Described by patients as “brain fog”.
5. Behavioral effects are common in many patients. Many have been or will be diagnosed as Attention Deficit Disorder, Attention Deficit Hyperactivity Disorder, Bipolar Disorder, or Obsessive-Compulsive Disorder. A minority do not show this pattern. Almost all, if previously seen by well-read physicians without prolonged observation, will have been labeled as “Delusional Parasitosis”. Temporal relationship to skin lesion onset is not known.
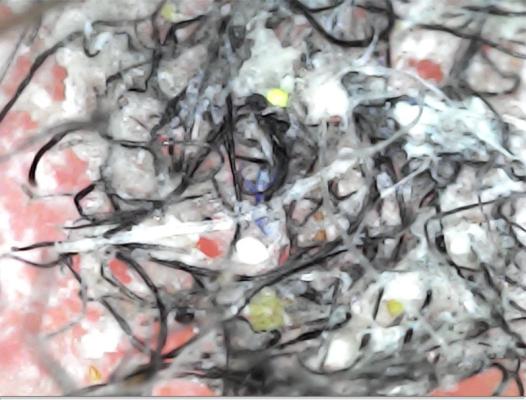
6.”Fibers” are reported in and on skin lesions. They are generally described by patients as white, but clinicians also report seeing blue, green, red, and black fibers, that fluoresce when viewed under ultraviolet light (Wood’s lamp). Objects described as “granules”, similar in size and shape to sand grains, can occasionally be removed from either broken or intact skin by physicians, but are commonly reported by patients. Patients report seeing black “specks” or “dots” on or in their skin, as well as unusual 1-3 mm “fuzzballs” both in their lesions and on (or falling from) intact skin.
OTHER COMMONLY REPORTED SYMPTOMS AND SIGNS
1. Change in visual acuity.
2.Numerous neurological findings. A variety of neurological symptoms have been reported. Some patients have been diagnosed with Amyotrophic Lateral Sclerosis, Multiple Sclerosis, and other well-known and recognized disorders, while others display significant symptoms not falling into any well-defined neurological category.
3. Gastrointestinal symptoms, which may include dyspepsia, gastroesophageal reflux, and/or changes in bowel habits often similar to Irritable Bowel Syndrome.
4. Neuropsychiatric symptoms and signs, ranging from mood or personality changes to diagnosed disorders including Attention Deficit Disorder, Bipolar Disorder, Obsessive Compulsive Disorder and occasionally frank psychosis. Temporal relationship to skin lesion onset is not known
5. Acute changes in skin texture and pigment. The skin is variously thickened and thinned, with an irregular texture and irregular hyperpigmentation pattern. The changes resemble age associated sun-exposure skin damage, but typically appear acutely
6. Skin examination often reveals excoriated and/or crusted lesions which, on examination with lighted magnification, are seen to have inclusions of variously colored (white, blue, black, or red) fibers. Skin examination may also reveal multiple hyper-pigmented macules, and an increase of what appears to be villous hair on arms and face.
7.Arthralgias are reported by many patients.
8. Associated diagnoses which have been commonly reported in this patient population include Borreliosis (better known as Lyme Disease), Fibromyalgia, and Chronic Fatigue Syndrome.
OTHER COMMONLY REPORTED OBSERVATIONS
1. Most patients will have sought care from multiple medical care providers. A large number will have been diagnosed with Delusional Parasitosis likely because of the juxtaposition of unexplained skin lesions and sensations and psychiatric overlay. Unfortunately, almost none will have received an appropriate diagnostic physical examination (particularly a microscopic or biopsy examination of lesions), but will have been diagnosed by history alone with grossly incomplete observation.
2. Most of these patients feel abandoned by the traditional medical care system and have sought alternative care providers or have self medicated, seriously compounding an already difficult medical situation
LABORATORY AND OTHER DIAGNOSTIC EVALUATION
To date, there have been no formal laboratory or imaging studies done in this patient group. There are some reasonably consistent clinical findings, however, that need further examination, in controlled studies, to be corroborated or refuted.
Morgellons
Morgellons Disease Case Definition
To: Centers for Disease Control and Prevention (CDC)
From: Morgellons Research Foundation
Date: February 14, 2006
Subject: CASE DEFINITION – MORGELLONS DISEASE (DRAFT)
The following case definition of Morgellons disease has been developed by physicians on the medical advisory board of the Morgellons Research Foundation. This case definition is a preliminary and evolving document, now updated for review by the Centers for Disease Control and Prevention (CDC). This document will be refined as further information becomes available and as members of the medical advisory board deem necessary.
The Following Six Signs or Symptoms Are The Basis of Morgellons Disease
1. Skin lesions, both spontaneously appearing and self-generated, with intense itching. The former may initially appear as “urticarial-like”, or as “pimple-like” with or without a white center. The latter appear as linear or “picking” excoriations. Even when not self-generated, lesions often progress to open wounds that heal abnormally and usually incompletely. (e.g., heal very slowly with discolored epidermis or seal over with a thick gelatinous outer layer.)
2. Crawling sensations, both within and on the skin surface. Often conceptualized by the patient as “bugs moving, stinging or biting” intermittently. Besides the general dermis, may also involve the scalp, nares, ear canal, and body hair or hair follicles. The sensations are at times related to the presence of easily seen insects, arthropods, and other human and non-human associated parasites that require serious attention from the observing clinician.
3. Fatigue significant enough to interfere with the activities for daily living.
4.Cognitive difficulties, including measurable short term memory and attention deficit, as well as difficulty processing thoughts correctly. Described by patients as “brain fog”.
5. Behavioral effects are common in many patients. Many have been or will be diagnosed as Attention Deficit Disorder, Attention Deficit Hyperactivity Disorder, Bipolar Disorder, or Obsessive-Compulsive Disorder. A minority do not show this pattern. Almost all, if previously seen by well-read physicians without prolonged observation, will have been labeled as “Delusional Parasitosis”. Temporal relationship to skin lesion onset is not known.
6.”Fibers” are reported in and on skin lesions. They are generally described by patients as white, but clinicians also report seeing blue, green, red, and black fibers, that fluoresce when viewed under ultraviolet light (Wood’s lamp). Objects described as “granules”, similar in size and shape to sand grains, can occasionally be removed from either broken or intact skin by physicians, but are commonly reported by patients. Patients report seeing black “specks” or “dots” on or in their skin, as well as unusual 1-3 mm “fuzzballs” both in their lesions and on (or falling from) intact skin.
OTHER COMMONLY REPORTED SYMPTOMS AND SIGNS
1. Change in visual acuity.
2.Numerous neurological findings. A variety of neurological symptoms have been reported. Some patients have been diagnosed with Amyotrophic Lateral Sclerosis, Multiple Sclerosis, and other well-known and recognized disorders, while others display significant symptoms not falling into any well-defined neurological category.
3. Gastrointestinal symptoms, which may include dyspepsia, gastroesophageal reflux, and/or changes in bowel habits often similar to Irritable Bowel Syndrome.
4. Neuropsychiatric symptoms and signs, ranging from mood or personality changes to diagnosed disorders including Attention Deficit Disorder, Bipolar Disorder, Obsessive Compulsive Disorder and occasionally frank psychosis. Temporal relationship to skin lesion onset is not known
5. Acute changes in skin texture and pigment. The skin is variously thickened and thinned, with an irregular texture and irregular hyperpigmentation pattern. The changes resemble age associated sun-exposure skin damage, but typically appear acutely
6. Skin examination often reveals excoriated and/or crusted lesions which, on examination with lighted magnification, are seen to have inclusions of variously colored (white, blue, black, or red) fibers. Skin examination may also reveal multiple hyper-pigmented macules, and an increase of what appears to be villous hair on arms and face.
7.Arthralgias are reported by many patients.
8. Associated diagnoses which have been commonly reported in this patient population include Borreliosis (better known as Lyme Disease), Fibromyalgia, and Chronic Fatigue Syndrome.
OTHER COMMONLY REPORTED OBSERVATIONS
1. Most patients will have sought care from multiple medical care providers. A large number will have been diagnosed with Delusional Parasitosis likely because of the juxtaposition of unexplained skin lesions and sensations and psychiatric overlay. Unfortunately, almost none will have received an appropriate diagnostic physical examination (particularly a microscopic or biopsy examination of lesions), but will have been diagnosed by history alone with grossly incomplete observation.
2. Most of these patients feel abandoned by the traditional medical care system and have sought alternative care providers or have self medicated, seriously compounding an already difficult medical situation
LABORATORY AND OTHER DIAGNOSTIC EVALUATION
To date, there have been no formal laboratory or imaging studies done in this patient group. There are some reasonably consistent clinical findings, however, that need further examination, in controlled studies, to be corroborated or refuted.
William T. Harvey, MD, MPH
Michael Ledtke, MD
Ginger Savely, RN, FNP-C
Raphael B. Stricker, MD
Gregory V. Smith, MD, FAAP
[img][img][/img][/img]